



Do you fit into one of these hEDS clusters?
Phenotypic Clusters and Multimorbidity in Hypermobile Ehlers-Danlos Syndrome

A recent study led by PhD Student, Taylor Petrucci, in the lab of Dr. Chip Norris at the Medical University of South Carolina looked at 2,149 patients and their symptoms, unveiling three patient clusters. A fully summary of the article can be found here.
Participants were asked about specific hEDS diagnostic criteria phenotypes and commonly associated comorbid conditions. This included things like Beighton score, various signs and symptoms included in the 2017 hEDS diagnostic criteria, and commonly reported comorbidities in hEDS like dysautonomia and mast cell activation syndrome.

The clusters identified are summarized below.
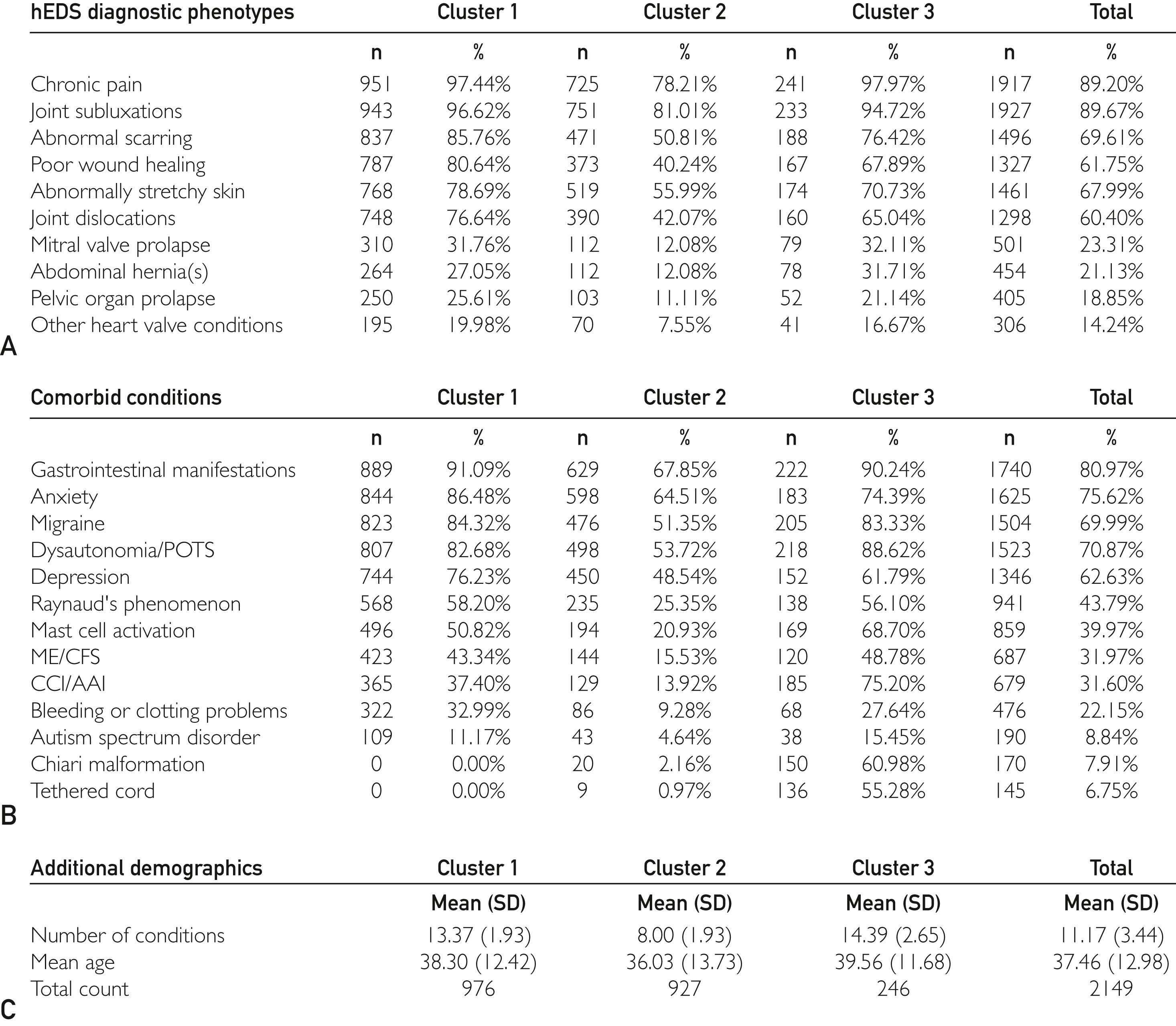
Cluster 1:
Higher prevalence of most diagnostic and comorbid phenotypes
Low prevalence of neurologic conditions such as craniocervical instability/atlantoaxial instability, Chiari malformation, and tethered cord syndrome.
Cluster 2
Lower prevalence of most phenotypes
Low prevalence of neurologic conditions such as craniocervical instability/atlantoaxial instability, Chiari malformation, and tethered cord syndrome.
Cluster 3
Intermediate phenotype presentation.
Higher rates of neurologic comorbidities like craniocervical instability/atlantoaxial instability, Chiari malformation, and tethered cord syndrome.
Increased prevalence of Mast Cell Activation Syndrome (MCAS).
Highest number of conditions, exceeding 14 in many cases.
Clusters did not correlate to degree of hypermobility, as measured by the Beighton score. Additionally, these clusters did not consider the severity of different symptoms, but only the presence or absence of the conditions asked about. So while cluster 3 reported more conditions, it does not necessarily mean those who fall within this cluster are “more severe” than other clusters.
I’m curious, if you have hEDS, what cluster, if any, do you feel best describes you?
Why do the clusters matter?
hEDS is often viewed as a “catch all” for anyone with generalized joint hypermobility and additional signs of a connective tissue disorder, that doesn’t fit phenotypically or genetically into other types of EDS or other connective tissue diseases. The spectrum in presentation can be really broad from one hEDS patient to the next, and this study certainly did not capture every possible phenotype or associated comorbidity!
The identification of clusters within the hEDS patient population provides valuable insights into the diversity of phenotypes and comorbid conditions, which can significantly enhance clinical care and research. By understanding these clusters, clinicians can tailor treatment plans more effectively, addressing the specific needs of each subgroup. Additionally, pairing phenotypic data like this with genetic information could lead to the discovery of specific genetic markers associated with certain clinical presentations, improving the accuracy of hEDS diagnoses and the development of future therapies.
This study also highlights that traditional diagnostic tools, such as the Beighton score and 2017 diagnostic criteria, may not reliably capture the full spectrum of hEDS phenotypes, underscoring the need for revised diagnostic criteria that better reflect the complexity of the condition, the EDS society is one group working on this right now.
Reference: Petrucci T, Barclay SJ, Gensemer C, et al. Phenotypic Clusters and Multimorbidity in Hypermobile Ehlers-Danlos Syndrome. Mayo Clin Proc Innov Qual Outcomes. 2024;8(3):253-262. Published 2024 May 15. doi:10.1016/j.mayocpiqo.2024.04.001
THIS is what I've been wanting to see discussed!! I am definitely cluster three. I just barely met the diagnostic criteria for hEDS and got diagnosed in 2022 and was then diagnosed with 10+ other conditions including CCI/AAI, occult tethered cord, and IIH. I think this is so so important because 99% of doctors will not consider these neurological/spinal conditions when they hear of an hEDS diagnosis and the patients are left with the responsibility to discover these things on our own, do our own research, put the pieces together and most likely travel out of state to get care which is a HUGE burden and totally inaccessible for many people who can't afford to do, can't take the time off work, or are too debilitated. And these conditions are very debilitating and often progressive (hEDS is obviously not progressive but OTC for example is). I'm thankful for social media and support groups for helping me figure out I had these conditions but it would be great if my hEDS diagnosis was a flag to be screened for these things so I didn't have to be my own doctor 24/7!
Another thing worth noting is that not only is the Beighton scale sometimes unreliable but diagnostic criteria such as chiari malformation, CCI, AAI and MCAS, MCAD are such specific diagnostics that so many of us, if we have gotten through the hurdles of getting diagnosed, we still may absolutely have no access at all to these kinds of tests. Insurance hurdles and the economics of it all can literally mean our care ends here, right outside the diagnostic line. This has the power to skew data, too. There’s so much work to be done.