



A New Clinical Study on Hypermobile Ehlers-Danlos Syndrome
"Phenotypic Clusters and Multimorbidity in Hypermobile Ehlers-Danlos Syndrome"

I am excited to share this new publication that I was a part of (congratulations to PhD student, Taylor Petrucci, on her work leading this study!).
We conducted a retrospective clinical study of 2149 patients, unveiling three distinct patient clusters based on multimorbidity patterns. Our findings suggest potential revisions to diagnostic criteria and emphasize the need for comprehensive multidisciplinary care in managing hEDS. Check out the full study for insights into hEDS clinical presentations and improving diagnostic and treatment guidelines!
As a disclaimer, it's worth noting that this study is derived from our genetic registry, where patients consented to participate in our research aiming to uncover the genetic underpinnings of hEDS. While we're eagerly awaiting the publication of our genetic findings, it's essential to acknowledge that genetic and biological studies entail substantial time and coordination. In the meantime, we felt it was important to share the valuable clinical insights gleaned from our genetic registry through this exciting new paper! Stay tuned for updates on our genetic research, hopefully available on a preprint server soon.

https://www.mcpiqojournal.org/article/S2542-4548(24)00024-9/fulltext#appsec1
The Ehlers-Danlos syndromes (EDS) are a group of 14 heritable connective tissue disorders. Hypermobile Ehlers-Danlos syndrome (hEDS) is the most prevalent subtype but lacks a clear genetic marker. Diagnosis of hEDS relies on criteria including generalized joint hypermobility (GJH), assessed by the Beighton score, systemic manifestations of a connective tissue disorder (CTD), and the exclusion of other CTDs.
Patients with hEDS often present with musculoskeletal pathologies, mild skin involvement, and a range of additional symptoms such as gut-brain axis disorders, sleep disturbances, anxiety, depression, fatigue, dysautonomia, mast cell activation syndrome (MCAS), and spinal instabilities. Symptom severity and the presence of comorbidities can vary widely.
This retrospective study analyzed a cross-sectional cohort of 2,149 clinically diagnosed hEDS patients in the United States to explore the prevalence of hEDS phenotypes and comorbid conditions and their relationships. By thoroughly understanding the associated comorbidities and clinical presentations, the study aimed sheds light on specific hEDS phenotypes and clinical presentation beyond what is evaluated in the current diagnostic criteria.
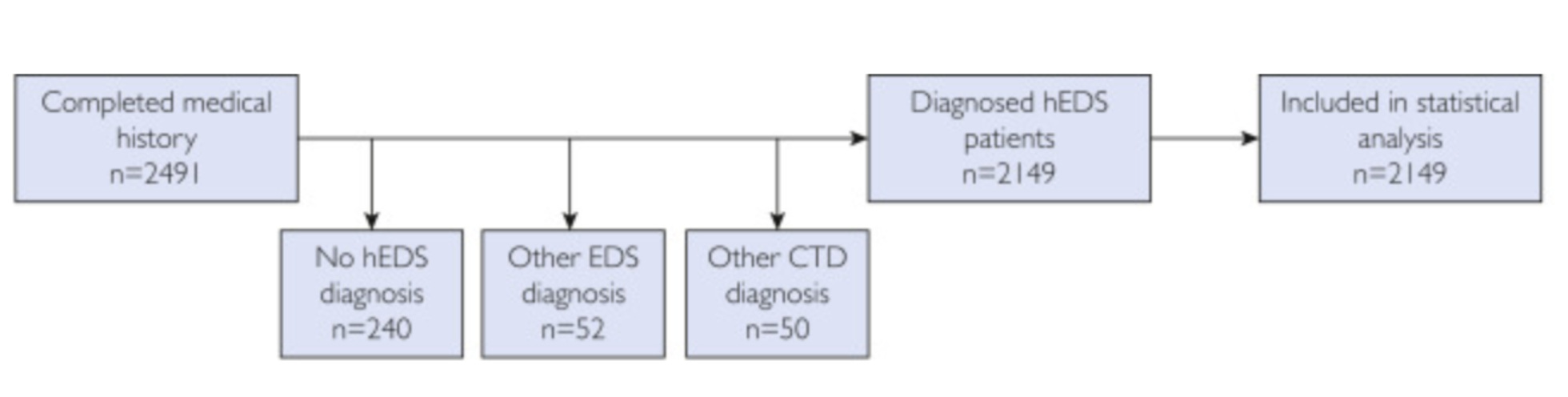
The study recorded self-reported responses from 2,491 participants enrolling in a hypermobile Ehlers-Danlos syndrome (hEDS) genetic research study. Participants were required to be over 12 years old, have a clinical diagnosis of hEDS from a physician, and reside in the United States. The study excluded individuals without an hEDS diagnosis, those diagnosed with another subtype of EDS, or another type of connective tissue disorder, resulting in 2,149 participants.
Data collected included basic demographic characteristics and hEDS signs and symptoms based on the 2017 hEDS diagnostic criteria, including the Beighton score, a tool used to assess generalized joint hypermobility (GJH). It also included information on comorbidities in patients with hEDS.

The majority of participants (91.53%) identified as female, 94% self-identified as white, and the average age was 37 years, with 76% reporting a family history of hEDS. Participants provided self-reported clinical information, categorized by gender, presence of hEDS symptoms, and common comorbidities.

In females, the most common issues were chronic pain and joint subluxations (over 90%), followed by abnormal scarring, stretchy skin, poor wound healing, and joint dislocations. The nonbinary cohort's phenotypes were similar to females, while males reported lower prevalence for most conditions.
Gastrointestinal issues were the most frequently reported comorbidity across all genders, with other common comorbidities including dysautonomia, POTS, anxiety, migraines, and depression, particularly prevalent among females and nonbinary individuals. Among female participants, the most common issues were chronic pain and joint subluxations, followed by abnormal scarring, stretchy skin, poor wound healing, and joint dislocations. The nonbinary cohort's phenotypes were similar to females, while males reported lower prevalence for most conditions. Participants reported an average Beighton score of 7.4 and typically had multiple comorbid conditions, with 98.6% reporting at least four.

Cluster variant analyses of hEDS patients revealed three distinct groups independent of age. Clusters 1 and 3 included patients with more than 11 conditions, while Cluster 2 had fewer than 11 conditions. Cluster 1 had a higher prevalence of most diagnostic and comorbid phenotypes, Cluster 2 had the lowest prevalence, and Cluster 3 exhibited intermediate phenotype presentations, with notable distinctions in neurologic comorbidities and MCAS prevalence. Integrating Beighton scores into the analysis dissolved these clusters, suggesting Beighton criteria may not effectively capture the spectrum of hEDS multimorbidity.


This study investigates the diverse phenotypic presentations and coexisting health conditions observed in patients with hypermobile Ehlers-Danlos syndrome (hEDS). The low prevalence of certain 2017 diagnostic phenotypes in our cohort, alongside the high prevalence of symptoms not covered in the 2017 hEDS diagnostic criteria, highlights potential shortcomings in current diagnostic guidelines and underscores the need for revisions to better encompass the full spectrum of hEDS manifestations.
The study identified three distinct disease clusters within the hEDS patient cohort based on the prevalence of comorbid conditions and diagnostic phenotypes. Interestingly, integrating Beighton scores into the clustering analysis dissolved the established clusters, suggesting that the Beighton score is not reliable for predicting patient phenotypes, comorbidities or severity.
The study underscores the importance of multidisciplinary approaches and collaboration among healthcare professionals, patients, and researchers to improve screening, diagnosis, and treatment for individuals with hEDS, potentially leading to significant enhancements in patient outcomes and overall quality of life.
Reference:
Petrucci, T., et al. (2024). "Phenotypic Clusters and Multimorbidity in Hypermobile Ehlers-Danlos Syndrome." Mayo Clinic Proceedings: Innovations, Quality & Outcomes 8(3): 253-262.
I hope you don't mind me asking a few questions. I've read through this a couple of times, but I'm still having a bit of trouble understanding the implications and how we should use this information.
Is it suggesting that there might be multiple types of HEDS now?
Are there symptoms mentioned that aren’t part of the current diagnostic criteria but should be considered?
Do the clusters help explain the genetic results or other possible causes?
As a patient, should I be looking to figure out which cluster I might fall into (if that's even the point)?
Great work and thanks for sharing. Interesting expressions in the 3 clusters. Looking forward to more studies like this as we await the genetic results. Hope you're having a good weekend.